
 BioDiaspora, a start-up company based on the research of company founder, Dr. Kamran Khan of St. Michael’s Hospital, has identified two mass gatherings in the Islamic world as key possible spread points for the life-threatening MERS coronavirus, which emerged in the Middle East in early 2012.
BioDiaspora, a start-up company based on the research of company founder, Dr. Kamran Khan of St. Michael’s Hospital, has identified two mass gatherings in the Islamic world as key possible spread points for the life-threatening MERS coronavirus, which emerged in the Middle East in early 2012.
BioDiaspora’s disease-tracking platform, which correlates uses global air traffic patterns to predict the international spread of infectious disease (as described in the original media release from St. Michael’s Hospital):
The first is umrah, a pilgrimage that can be performed at any time of year but is considered particularly auspicious during the month of Ramadan, which this year began on July 9 and ends on Aug. 7. The second is the hajj, a five-day pilgrimage required of all physically and financially able Muslims at least once in their life. It takes place Oct. 13 to 18 this year and is expected to draw more than 3 million people.

It also identified the Mumbai-India corridor as particularly vulnerable to MERS based on the predicted exit traffic of travelers leaving the hajj and returning to their home countries following the mass religious event.
Khan’s research findings, published in PLOS Currents: Outbreaks, have attracted media coverage from the Times of India, CanIndia, Toronto Star‘s Foreign Desk blog (Jennifer Yang), Science Daily.com, DowntoEarth.org and Homeland Security News Wire.
Here’s an excerpt from the original release:
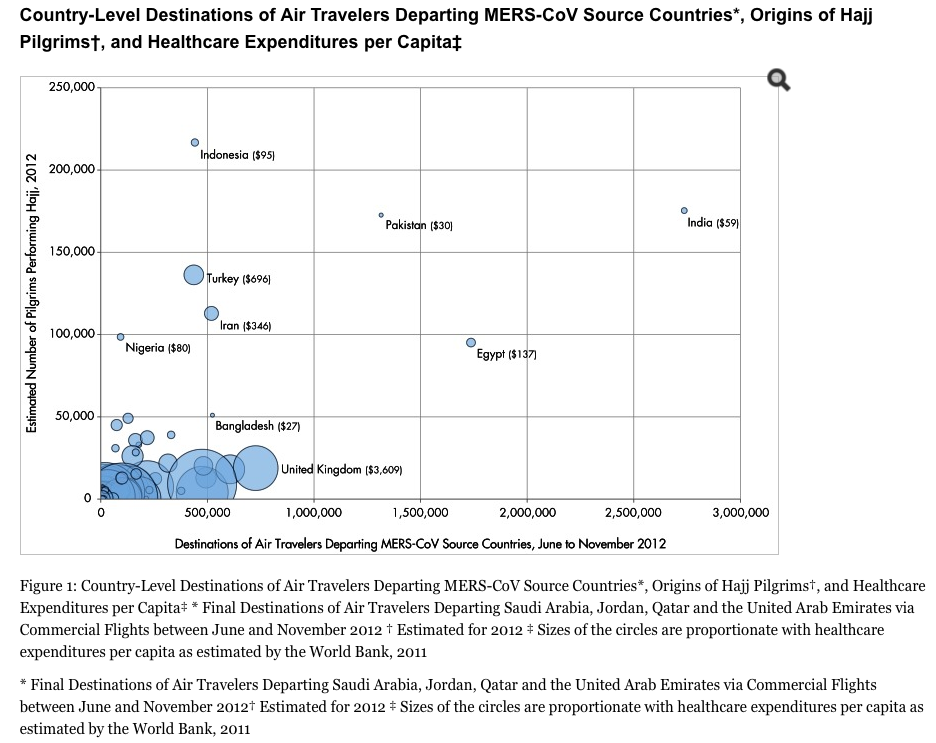
Dr. Khan’s team analyzed 2012 worldwide airline traffic and historic hajj data to predict population movements in and out of Saudi Arabia and the broader Middle East during these two mass gatherings to help countries assess their potential for MERS introduction via returning travelers and pilgrims. He also used World Bank economic and per capita health care expenditure data to help gauge individual countries’ abilities to detect imported MERS in a timely manner and mount an effective public health response.
Results of the study were published in the online journal PLoS Currents: Outbreaks.
Dr. Khan, an infectious disease physician, is the founder of BioDiaspora, a web-based technology that uses global air traffic patterns to predict the international spread of infectious disease. The BioDiaspora platform has been used by numerous international agencies, including the U.S. Centers for Disease Control and Prevention, the European Centre for Disease Prevention and Control and the World Health Organization to evaluate emerging infectious disease threats, including those during global mass gatherings such as the Olympics and the hajj.
“With millions of foreign pilgrims set to congregate in Mecca and Medina between Ramadan and the hajj, pilgrims could acquire and subsequently return to their home countries with MERS, either through direct exposure to the as-of-yet unidentified source or through contact with domestic pilgrims who may be infected,” he said.
Dr. Khan’s team found that of the 16.8 million travelers who flew on commercial flights out of Saudi Arabia, Jordan, Qatar and the United Arab Emirates between June and November 2012 (the period starting one month before Ramadan and ending one month after the hajj) 51.6 per cent had destinations in just eight countries: India (16.3 per cent), Egypt (10.4 per cent), Pakistan (7.8 per cent), Britain (4.3 per cent), Kuwait (3.6 per cent), Bangladesh (3.1 per cent), Iran (3.1 per cent) and Bahrain (2.9 per cent).
Twelve cities–Cairo, Kuwait City, London, Bahrain, Beirut, Mumbai, Dhaka, Karachi, Manila, Kozhikode (India), Istanbul and Jakarta–each received more than 350,000 commercial air travelers between June and November 2012 from the four countries where MERS cases have been traced back to. In contrast to SARS, where the disease was introduced into predominantly high-income countries through air travel, more than half of all air travelers departing Saudi Arabia, Jordan, Qatar and UAE have final destinations in low or lower-middle income countries. Two-thirds of all hajj pilgrims originate from low or lower-middle income countries.
Of particular note is the degree of connectivity between the Middle East and South Asia. Collectively, India, Pakistan, Bangladesh, Afghanistan and Nepal represent the final destinations of nearly one-third of all international air travelers departing Saudi Arabia, Jordan, Qatar and the UAE, and the origins of roughly one in four foreign hajj pilgrims worldwide.
“Given that these countries have limited resources, they may have difficulty quickly identifying imported MERS cases, implementing rigorous infection control precautions and responding effectively to newly introduced cases,” Dr. Khan said.
Dr. Khan’s previous research suggests that if screening of air travelers for MERS is considered, it would be far more efficient and less disruptive to the world’s air traffic to screen travelers as they leave source areas in the Middle East rather than screen the same travelers as they arrive at other airports around the world. However, all countries receiving pilgrims and other travelers from known MERS areas should mobilize their infectious disease surveillance and public health resources in ways that are commensurate with their potential for MERS introduction, he said.
The full text is available on St. Michael’s Hospital newsroom.
Posted by Elizabeth Monier-Williams, marketing and communications manager.